
Home > Publications > Policy Briefs > 3/ Feeding of young children, a medium of their learning and their social (...)
– Children’s feeding is not only determined by their nutritional needs. The diet diversification stages, and the transition to solid foods and to the adult meal, are also strongly influenced by social issues: food is a support of the social learning for children, and of their integration in the adult world.
– The way in which the child’s body is seen by those around it, also determines the choice of foods for the child. To understand that research on feeding of the baby is indissociable with research on the social and cultural-related issues is decisive in order to understand the decisions and choices made by the mothers in feeding their child.
In Cameroon in 2008, almost 40% of households lived below the poverty threshold (ECAM 3, 2008). In this socioeconomic context, 33% of the children from 0 to 59 months suffered from chronic malnutrition and 70% of children were anaemic (27% in a minor form, 31% moderately, and 2% seriously) (EDS, 2011). The nutrition and health of children from 0 to 5 years of age is therefore a major issue for public health policies. Breastfeeding infants is a feeding practice which is generally valued highly, since almost all mothers use it, but contrary to the recommendations of the World Health Organisation (WHO), this breast-feeding is only exclusive for 20% of infants aged from 0 to 6 months (EDS, 2011). How can this “non-exclusive breastfeeding” of infants, sometimes from their youngest age, be explained? What are the real practices and representations of mothers today?
In anthropological literature on the feeding of children, dietary choices are essentially presented as being a social construct derived from medicinal discoveries as well as the daily constraints to which families are subjected, and as being at the heart of the values of a society at a given moment in its history. Works on infant health remain sparse, but the distinction between the “biological age” and the “social age” of the child explains the decisions which can be observed in the feeding of the latter. In a more general manner, decisions relating to what the child wants to / has to eat and its dietary pathway can be analysed as referring to the conceptions of the child in black Africa (Erny, 1987). The child passes through various statuses in its development. At its birth, it is an in-be-tween being because it has not yet broken with the world of the spirits, and continues to be a particular person within the family. The integration of the individual in its group is an issue relating to the health of the social group. The function of eating together which is fulfilled by feeding is revealing with respect to the child’s level of integration in the group. How is “social” life learnt through feeding? What are the “stages” of this learning process?
In order to answer these questions, the study which we have realised aims to characterise cultural practices of feeding of the child from 0 to 3 years, in particular the norms, practices and representations of feeding the latter. The age group between 0 and 3 years was selected for our study not only because it corresponds to a pivotal period in the education of taste for children, but also because it refers to a certain number of dietary norms in medical culture.
The feeding practices relating to the young child, and the development of the latter, are determined by a certain number of social factors. They are deter-mined by the “social age” of the child more than by its “biological age”, and need to contribute towards making the child a full member of its social group.
The body of the child is not just seen in a “biolog-ical” manner, but also in a “social” manner: by solid-ifying and by allowing and asking the child to eat the same dishes as the adults, this body integrates the child into the world of adults and makes of the child a “human” who is a full member of the family network.
The feeding of the child follows its social age more than its biological age. At the age of 12 months, the child must be able to walk like its peers. This presupposes passing through preliminary stages: sitting, crawling, the first growths of teeth, and finally walking. However, feeding contributes to the production of the body. Feeding practices are there-fore adapted to the child in order to offer it foods which allow it to follow the process of physiological toughening and finally to have the strength to walk, like any other member of the social group.
The study carried out in the two cities in Cameroon shows that social age is taken into account in the choices which mothers make, what-ever their social class. The taking into consideration of social age makes it possible to understand the decision-making processes which are carried out by mothers in the initiation of the children to local dietary models.
A dietary pathway which leads to the state of an adult, a member of the family
The dietary pathway of the child provides infor-mation on its future within the family. This pathway is composed of several “sequences” which the mothers describe as different stages of progressive integration of the child in the family circle and its socialisation through the foods which are offered to it.
From 0 to a few days old, the mother (generally) “gives her breast” to the child. Use of the term “breast” in the local language when referring to breastfeeding depicts the bodily contact between the mother and the child, which brings to mind the link which exists between the two when the child is still in in utero. Hence breastfeeding also provides evidence that the child is still in an intermediate phase between the body of its mother and society.
From 0 to 2 months, children are still fed with their mothers’ milk, but it may occur that other foods are added to this, in order to fill the child. Infants eat in the arms of their mother or any other experienced woman who is able to feed them with a bottle within their family network.
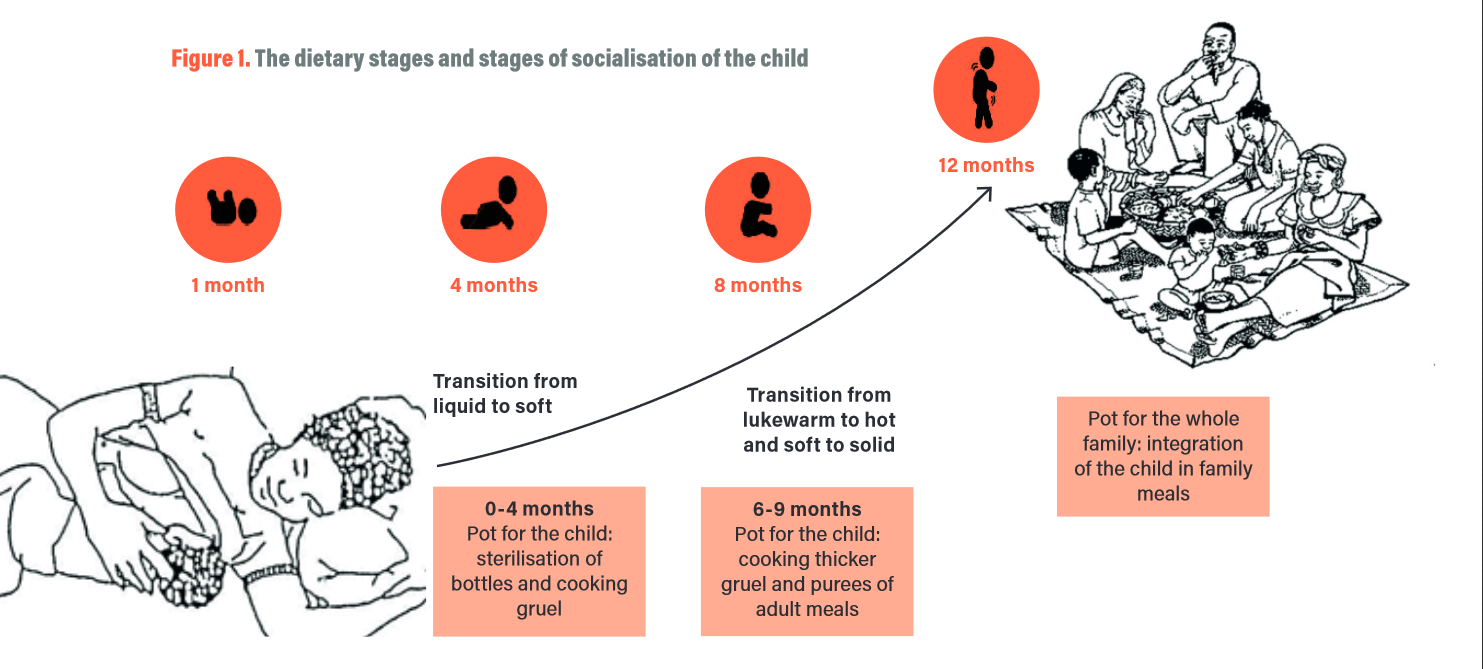
From 2 to 4 months, what “eating” means. From the age of 2 months, the mothers begin to space out the times of breastfeeding. They introduce liquid and semi-liquid gruels, and even crushed adults’ meals, in order to begin to familiarise the child with what it will eat when it is bigger. The introduction of adult meals also follows a conception according to which gruels and milk are not seen as nourishing foods, and so the consumption of these foods is not equated with “eating” by mothers and grandmothers.
From 4 to 6 months. With the resumption of their professional activity, the mothers are often forced to stop breastfeeding. Moreover, the fact that a child watches adults eating and putting the spoon to their mouth is interpreted as a desire to taste the adults’ meals. In all social classes, the age of 4 months there-fore signals the beginning of a dietary transition. The child sometimes tastes the adults’ meals and begins to learn to eat hot food.
From 6 to 9 months. From 6 months onwards, children begin to be weaned off breastfeeding. The purees and gruels which are served to them become progressively richer and “heavier”, and hotter in order to get closer to the meals which are traditionally valued in the society of Cameroon; soft, hot dishes are presented to the child. This kind of feeding confers to the child the status of a “human” and initiates it to the dietary heritage of its group, by presenting to it the foods which are representative of its ethnic identity.
From 9 months to 1 year. Between 9 months and 1 year, the weaning of the child takes place in the majority of households. The child therefore “eats”, with “eating” being understood as consuming the family dish, served hot. The child learns to use its hands to take its food, and hence progressively acquires its independence.
Finally, from one year onwards, the main meal of the child is the family meal. Feeding therefore no longer fulfils a solely biological function, but has a social function – allowing the child to sit at the table with and be integrated into its group.
The pot, a decisive object for the integration of the child in its group
One cultural object is at the heart of all of the dietary transitions through which the child passes, and plays a determining role in the integration of the latter in its group. It is the pot, the traditional container in which the meal of the group is cooked. While the child is young, its pot is used for sterilising bottles, and is stored separately from the other pots of the house. Symbolically, the child is not yet part of the social group. The pot in fact symbolises warmth and the social group, and the fact that the child eats foods from the same pot which feeds the other members of the social group signifies its passage from lukewarm to hot and confirms its integration in the group. Use of the pot is related with the group culture, since it is from this common recipient that the food is taken which the members of the family will share.
As a cultural artefact, the pot provides informa-tion, through its heat and the smells which it gives off, as well as the quantity of food which it contains, on its purpose: for the family or for the child. It there-fore provides information on the level of integration of the child in its social group. Serving a child from the same pot as the adults shows that the latter has left the aquatic world in order to become earth like the rest of the living.
In a general manner, the dietary pathway of the child is translated by the transition: 1) from body temperature (37°C) to lukewarm and then to hot; 2) from liquid to semi-liquid, to soft and then to solid; 3) from the individual pot (in order to heat water for the bottle or gruels) to the pot used for the family meal. A child who is integrated into its social group is therefore one who eats hot, cooked, solid food.
Obesity of the young child and the risk of social isolation”
According to what the mothers say, the figure of the child provides information on its state of health. However, the social norms with respect to the repre-sentation of the body of the child may be very far away from medical standards which consider the real weight of the child. Hence many mothers are happy about excess weight in the child, which is a safety margin for the event that the child contracts a disease such as malaria.
An overweight child is not considered as being in a “pathological” state unless the child becomes shapeless, and the various parts of its body are indis-tinct due to a dominance of fat. From being a “beau-tiful baby”, the obese child is then considered as “a burden”, and he becomes socially embarrassing.
Hence, contrary to the tradition according to which friends, acquaintances and relatives wish to carry a child as soon as they meet it, those around it refuse to carry a child which is significantly over-weight. One of the risks is therefore of the social isolation of mothers whose children are significantly overweight.
Moreover, carrying the child plays a role in the socialisation of the child because it creates a link between the child and its carrier (the affective role), and because it is also a way for the adult to be able to lead the child into places where it will meet other people. Hence, beyond individual and medical aspects, with the state of the child’s body being a danger for its survival, on the social level, the weight of the child may be a hindrance to the development of social relations and lead to its isolation. Feeding, which is an element of socialisation, in this case leads to the isolation of the child and its mother. And so that the child can return to socially accepted norms, the mothers need to apply therapies consisting of changing the quantity and quality of food given to the child.
The results of our study on the practices and representations of mothers with respect to how they feed their young child display that the dietary pathways
(including the products and utensils used) of children are determined more by their social age than their biological age. Feeding is at the heart of the integration of the young child, and must also allow it to learn the dietary repertoire of its group. It must therefore be ensured that feeding training programs aimed at the mothers do not make reference solely to the biological age of the child, but also to its social age.
Moreover, the relationship with the body, and particularly the way in which the child is seen by those around it, also determines the choice of foods for the child. A “beautiful” baby is an overweight baby, and an overweight baby is not considered to be “ill” unless it is no longer possible to carry it, and its weight therefore becomes a constraint to social relations.
In view of the data gathered within the framework of this study, it can therefore be observed that research on the feeding of the baby remains indissociable with research on the social and cultural representations of the body of the baby, on the one hand, and on the other hand the identity-related issues which determine food choices for the child. This information is in fact decisive in order to understand the decisions made by the mothers in feeding their child.
– Estelle KOUOKAM, Catholic University of Central Africa, Cameroon
– Anne BERCHON, CIRAD, Montpellier, France
Erny, P. (1987). L’enfant et son milieu en Afrique noire : essais sur l’éducation traditionnelle. Paris. L’Harmattan.
Institut national de la statistique (2008). Tendances, profil et détermi-nants de la pauvreté au Cameroun en 2007. Rapport provisoire ECAM 3, 16 p.
Institut National de la Statistique (2011). Enquête Démographique et de Santé et à Indicateurs Multiples EDS-MICS. Yaoundé, Cameroun
